My Voice Matters
Lulu Luckock of Lulu Luckock Counselling reveals the ways in which we, as parents, can give our children a voice by ensuring we are listening ... Read Feature

In the emergency treatment of ill or injured patients, oxygen has always been a major component. It is widely believed that oxygen eliminates breathlessness and cures dyspnoea. This belief is incorrect. Administration of Oxygen is often not from necessity but for the pure and simple fact that we can.

A search through relevant medical literature will reveal only three documented benefits of Oxygen:
Other than these three conditions there is no documented evidence in the scientific or medical literature that supports Oxygen administration. There is, however, plenty of evidence documenting reactive Oxygen species and free radicals resulting in negative patient outcomes. Oxygen it seems is very much a double-edged sword that can be invaluable when administered correctly yet detrimental when administered inappropriately.

Oxygen is a very unstable element, highly reactive and supports combustion. It is a diatomic gas, colourless, odourless, tasteless and has an atomic number of 15.9994 g-1. 29.95% of the earth’s atmosphere is composed of Oxygen and it is the third most abundant element in the universe. Oxygen is an essential element for human life.
Oxygen tanks are supplied in different sizes. The most commonly used portable cylinder is the C/D cylinder. It is pressurised to 2000 psi and contains 450L of Oxygen when full. Oxygen tanks should only be cleaned with soap and water. Oil and petroleum-based products should be stored away from cylinders at all times. The gauge found on the side of the tank should be checked and a cylinder should be replaced if the needle points to the red zone. Prior to administration the dial on the side of the tank should be turned to the fully “ON” position. The litre flow gauge is found on top of the cylinder and turned so that the appropriate litre flow desired is shown through the window. Oxygen tubing should be securely connected to the Christmas tree. For further information the following video is extremely informative on Oxygen tank usage.
Oxygen’s only true contra-indication is its use in explosive environments. Caution should be taken with its administration in the presence of fire at the scene of an incident and during defibrillation. Dosage often is guided using pulse oximetry when the use of ABGs are unavailable. Under normal circumstances a target Oxygen saturation of 94-98% is acceptable but those with pre-existing chronic respiratory disorders such as COPD or advanced cystic fibrosis a range of 88-92% is required. In short, when oxygen is administered it should be monitored using pulse oximetry.

Oxygen is a drug and requires a prescription in order to be administered. It is provided either as a compressed gas or in liquid form. It is administered to a patient via a regulator and flow meter by means of plastic tubing and an Oxygen mask, nasal cannula or bag valve mask. Guidelines for Oxygen administration are disseminated by the British Thoracic Society.
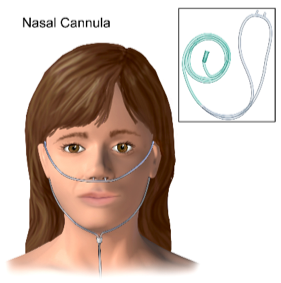
The nasal cannula can be used to administer low flow oxygen. 1-6 L/min is the administration range with an increase of 2-3% FiO2 (inhaled Oxygen) per litre. Administration of Oxygen via nasal cannula utilises the nasal cavity as a reservoir so it can be administered to patients predominantly breathing through their mouth as well as their nose.

The non-rebreather mask can be used to administer high flow oxygen. This would be required for the patient spontaneously breathing displaying signs and symptoms of hypoxia. It requires a flow rate of 12-15L/min and delivers approximately 80% FiO2. Prior to administration, the reservoir bag should be filled with Oxygen by place in a finger over the one-way valve. The reservoir bag should not completely empty when the patient inhales.

Both the nasal cannula and the non-rebreather mask are only effective when the patient is breathing. Should the patient lack sufficient respiratory effort to sustain life or become apnoeic (respiratory arrest) positive pressure ventilation must be initiated immediately. The self-inflating bag valve mask (BVM) is the instrument of choice. The bag valve mask can be used with Oxygen administered at 15L/min however if no Oxygen source is available it can be used with room air. It delivers approximately 80% FiO2 when utilised with an Oxygen source at 15L/min. In order to ventilate a patient effectively airway manoeuvres should be implemented, and a tight seal made between the patient’s face and the mask. A ventilation rate of one breath every 6 seconds is adequate and success can be seen when chest rise is observed. Although ventilation via BVM can be accomplished with one rescuer a greater success rate can be achieved with 2. One rescuer simply ensures an airtight seal between the mask and the patient’s face, the second squeezes the bag every 6 seconds.
This list is not exhaustive, and more guidance can be found at;
https://bnf.nice.org.uk/treatment-summary/oxygen.html
In conclusion, the days of oxygen administration purely because we think we should are long gone. The administration of Oxygen requires pulse oximetry (SpO2) monitoring. Its administration should be guided by these results however the limitations of pulse oximetry must be well understood.
Akero A, Christensen CC, Edvardsen A, et al. Hypoxaemia in chronic obstructive pulmonary disease patients during a commercial flight. Eur Respir J 2005;25:725–30.
Cottrell JJ, Lebovitz BL, Fennell RG, et al. Inflight arterial saturation: continuous monitoring by pulse oximetry. Aviat Space Environ Med 1995;66:126–30.
Hoffman CE, Clark RT, Brown EB. Blood oxygen saturations and duration of consciousness in anoxia at high altitudes. Am J Physiol 1946;145:685–92.
Alteiemer WA, Sinclair SE. Hyperoxia in the intensive care unit: why more is not always better. Curr Opin Crit Care 2007;13:73-78.
O’Connor RE, Brady W, Brooks SC, Diercks D, Egan J, Ghaemmaghami C, Menon V, O’Neil BJ, Travers AH and Yannopoulos D. 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science Part 10: Acute Coronary Syndromes. Circulation 2010; 122: S787-S817.
Ronning OM, Guldvog B. Should Stroke Victims Routinely Receive Supplemental Oxygen? A Quasi-Randomized Controlled Trial. Stroke 1999;30:2033-2037.
Rabi Y, Rabi D, Yee W: Room air resuscitation of the depressed newborn: a systematic review and meta-analysis. Resuscitation 2007;72:353-363.
Davis PG, Tan A, O’Donnell CP, et al: Resuscitation of newborn infants with 100% oxygen or air: a systematic review and meta-analysis. Lancet 2004;364:1329-1333.
Stockinger ZT, McSwain NE. Prehospital Supplemental Oxygen in Trauma Patients: Its Efficacy and Implications for Military Medical Care. Mil Med. 2004;169:609-612.
Austin MA, Wills KE, Blizzard L, Walters EH, Wood-Baker R. Effect of high flow oxygen on mortality in chronic obstructive pulmonary disease patients in prehospital setting: randomised controlled trial. BMJ 2010;341:c5462.
Kilgannon JH, Jones AE, Parillo JE, at al. Emergency Medicine Shock Research Network (EMShockNet) Investigators. Relationship between supranormal oxygen tension and outcome after resuscitation from cardiac arrest. Circulation 2011;14:2717-2722.
Harten JM, Anderson KJ, Kinsella J, et al. Normobaric hyperoxia reduces cardiac index in patients after coronary artery bypass surgery. J Cardiothorac Vasc Anesth 2005;19:173–5.
McNulty PH, et al. Effects of supplemental oxygen administration on coronary blood flow in patients undergoing cardiac catheterization. Am J Physiol Heart Circ Physiol 2005; 288: H1057-H1062.
Bledsoe BE, Anderson E, Hodnick R, Johnson S, Dievendorf E. Low-Fractional Oxygen Concentration Continuous Positive Airway Pressure Is Effective In The Prehospital Setting. Prehosp Emerg Care 2012;16:217-221.
Click here for more articles on Wellbeing
Lulu Luckock of Lulu Luckock Counselling reveals the ways in which we, as parents, can give our children a voice by ensuring we are listening ... Read Feature
Everyone is talking about it! Davina has done a programme about it and your friends have mentioned their symptoms. But how do you know if ... Read Feature
Never have we seen such a clear demonstration as to the importance of CPR and using a defibrillator, than watching Christian Eriksen being resuscitated on ... Read Feature




